Gilbert H.
From Benchmark to Best Practice: Reducing Blood Culture Contamination in Sepsis Care.
Poster: SHEA Spring Conference 2026.
April 2026
Background
Blood culture contamination (BCC) is a persistent problem in the hospital, contributing to unnecessary antibiotic exposure, excessive diagnostic testing, treatment delays, increased length of stay, and higher costs.
For patients with suspected or confirmed sepsis, BCC has particularly serious implications, as early identification of the causative pathogen and prompt initiation of appropriate antimicrobial therapy are critical.
National benchmarks define <3% contamination as acceptable, yet emerging evidence supports a more ambitious goal of ≤1%, particularly in high-risk populations such as patients with sepsis.
Starting in 2019, we implemented a change in our blood culture collection practice, including continuous monitoring of BCC rates.
Purpose & Aims
The purpose of this project was to evaluate the impact of the changes in our overall blood culture collection specifically for patients admitted with sepsis.
Methods
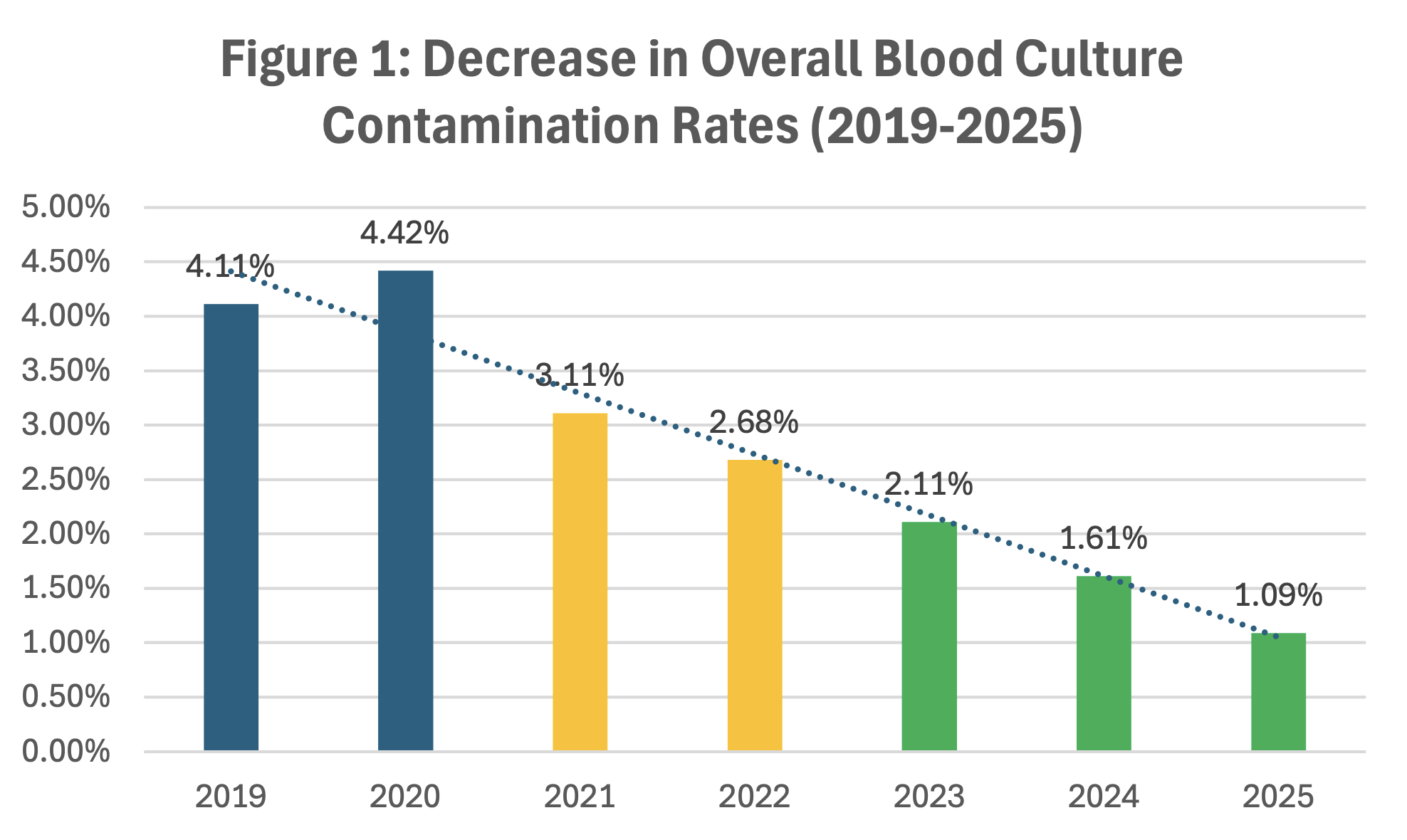
In our overall practice change for blood culture collection across three time periods, we achieved a 74% reduction in BCC (Figure 1).
- 2019-2020: No blood culture diversion used
- 2021–2022: Implementation of manual blood diversion device (BDD #1)
- 2023–present: Implementation of an automatic blood diversion device (BDD #2)
-
- 4. Data were extracted for adult patients admitted to the hospital who had a final discharge diagnosis of sepsis, regardless of their initial admission diagnosis.
Results
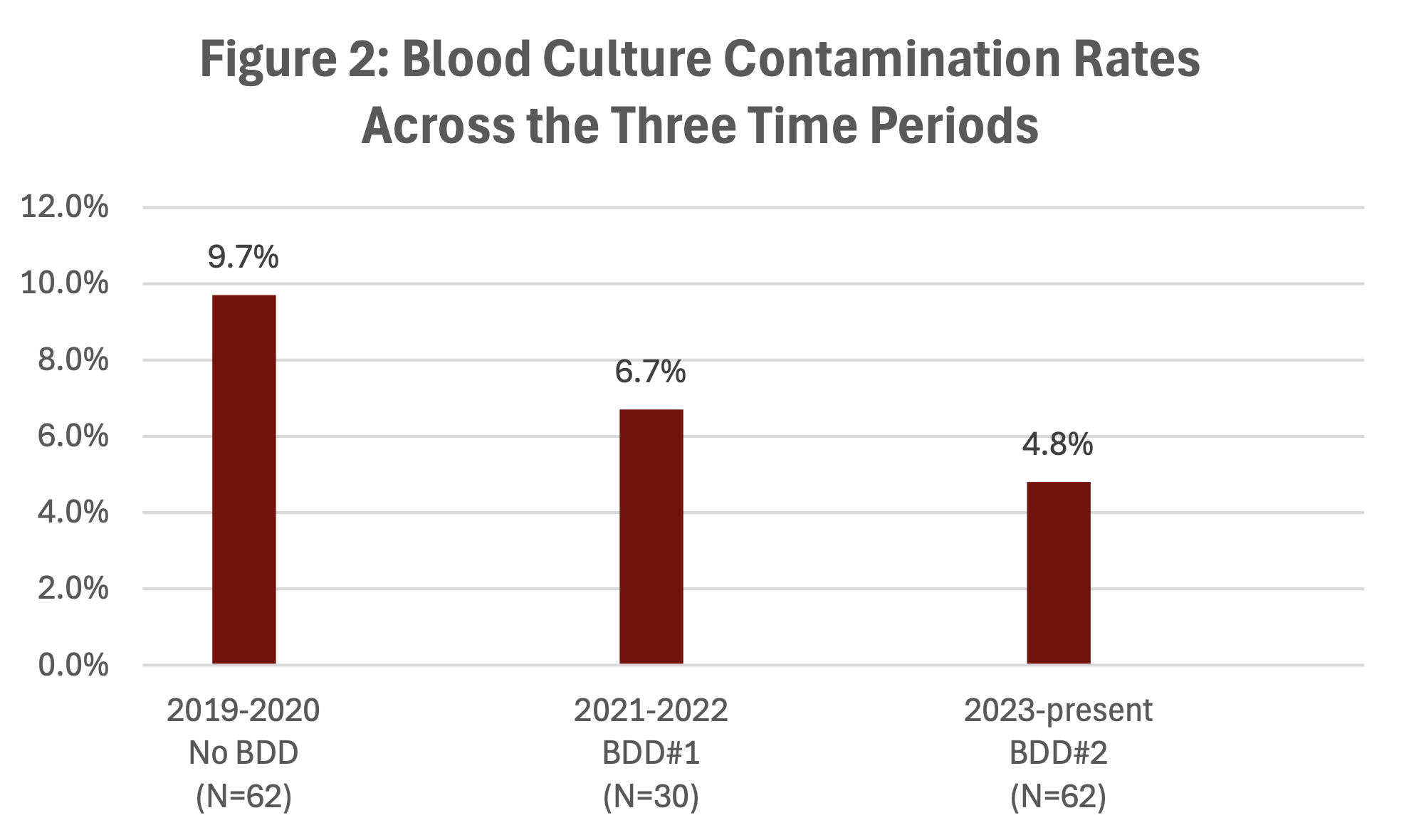
A total of 154 blood cultures in patients with a final discharge diagnosis of sepsis were reviewed across the three time periods, with BCC results displayed in Figure 2.
Additionally, manual BDD #1 was used in 48% (30/62) of the blood culture collections versus to 78% for automatic BDD #2, with staff feedback indicating greater ease of use with the automatic BDD #2 system.
Conclusions, Practice Implications & Future Research
Adoption of a BDD was associated with a 50% (9.7-4.8%) reduction in BCC, with the lowest rates following implementation of automatic BDD #2.
These findings underscore the importance of optimizing BCC practices as a key component of sepsis management, antimicrobial stewardship, and patient safety efforts.
Additional research is needed to identify strategies to further reduce BCC in sepsis patients, with particular attention to BDD workflow integration, and process adherence during real-world use.
Related Studies
No items found.